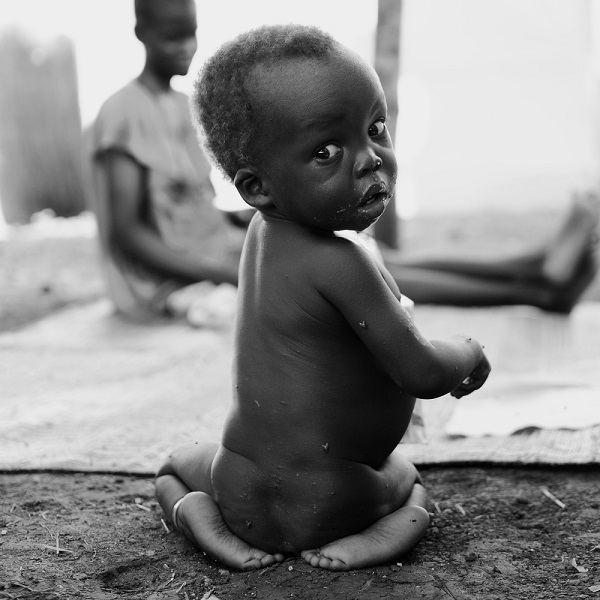
Photo by Mathieu Fortoul/MSF
OBGYN Rachel Chan Seay will hold a talk in Annapolis, Maryland, on October 21 in support of the Because Tomorrow Needs Her project. Dr. Seay has worked with Doctors Without Borders/Médecins Sans Frontières (MSF) in Sierra Leone and South Sudan, and she is a clinical instructor at the Johns Hopkins School of Medicine. Her research focuses on the history of medicine, strategies to decrease maternal mortality, and the designing of medical education curricula in global health.
In her talk, Dr. Seay will share her experiences in the field with MSF and discuss some of the challenges that women and girls face in trying to access the medical care that they need.
Where have your missions with MSF been and what has been your role in each?
My first mission with MSF was in Fall 2013. The project was in Bo, southeastern Sierra Leone, in a freestanding MSF maternal and pediatric hospital. I was there for about three months working on emergency obstetrics and maternal and child health with two other OBGYNs.
My next project, in South Sudan, was structured a bit differently. There, MSF runs the pediatric and maternity department within a larger government-run Ministry of Health hospital. At this project there is normally one OBGYN at a time who works with an ex-pat midwife, who is supervising and training a larger team of local midwives. My primary role in this project was to work with the midwives and to treat the patients who had complicated obstetrical or surgical cases.
You were recently honored as a 2015 Fellow in the History of American Obstetrics and Gynecology with the American Congress of OBGYN (ACOG). What has been the primary focus in your research to decrease maternal mortality?
Aside from my work with MSF, I’m very actively involved in global health and global health education. I’m on the faculty of Johns Hopkins University where I help with both the OBGYN resident and medical student electives and global health interest groups.
One of my particular areas of interest, both clinically and academically, revolves around the education, prevention and treatment of postpartum hemorrhage. My fellowship research project with ACOG is focusing on the history of the management of post-partum hemorrhage in the United States from approximately 1900-1940. I’m looking at the application of techniques and maneuvers that were used at that time and that might still be applicable in developing and low-resource settings.
In your work on the ground and in your research, what do you see as some of the biggest barriers facing women in terms of accessing medical care?
The issue of women accessing medical care in many MSF-based settings is a complicated and multi-factorial problem. While there are certainly problems in terms of just logistical access, including quality of roads, availability of transportation, and distance from home to a primary or tertiary center, there are also the issues of access related to the prioritization – or lack of prioritization – of women’s health care issues by governments, health administrations, and even health care workers.
Take for example, the issue of how ministries of health prioritize the importance of contraception and prenatal care and how this affects access to those services for women. Meanwhile, I think an additional barrier has to do with the availability of specialized care providers. There is a lack of medical education for general providers with some OBGYN experience and for those with specialty training in OBGYN and maternal health-related issues.
When have you seen these issues of access for women and girls arise in your missions with MSF?
It happens all the time, but there is one story that sticks out in my mind. While in Bo, we had two young girls, both 17, who started off on really parallel courses that ended dramatically differently. Both girls were pregnant with their first babies and had been laboring at home for several days with obstructed labor. Eventually, they each made their way out of the bush to a primary clinic where they were transferred to our facility. By the time one of the girls had arrived, her baby had died, while the baby of the other was still alive. Both girls delivered by C-section and ended up having really bad pelvic and abdominal infections. After about six to eight weeks in the hospital with us, the mother whose baby died ended up dying as well. The mother whose baby survived recovered and ended up doing well and being discharged.
The complications and suffering of both of these girls were happening at the same time – they even shared the same room! To me, this story paints such a stark picture of two different outcomes from a problem that is completely preventable. Both of these girls exemplify the incredible complication and suffering that can come from a lack of access to timely and appropriate medical care. We just don’t see this in developed countries because we have access to quality, timely care.
We also saw a lot of patients who developed obstetric fistulas after suffering from obstructed labor. While our project wasn’t specifically treating those with obstetric fistulas, we would often identify them and refer them to another NGO that was working in the area. Like many complications that I saw result in morbidity and mortality, obstetric fistula is an entirely preventable problem.
As mentioned, often times these issues aren’t as recognized in developed nations because the issue of access doesn’t exist to the same degree as it does in some other settings. What would you hope that people who come to your talk take away from it?
Partly just an expanded awareness of how fortunate we are to have access to medical care, contraception and preventative health care. I would like for the project to encourage people to take responsibility for their own preventative health care and encourage their families, friends and community to be involved as well. Prevention is always better than treatment.
I believe that the improvement of the global maternal health situation is truly an inter-disciplinary effort. And that’s why I’m not only doing talks at medical schools and schools for public health, but also at general universities, not specific to medical audiences.
I think it’s important to raise awareness that there is a need for a lot of different support and skill sets, whether it’s medical or engineering or education. There are many roles and skills needed to improve access to health-related services. I hope these talks will help illuminate these issues, update people about what is being done, and motivate people to get involved – whatever their skill
And I think that traveling abroad is not for everyone, and not everyone who attends these talks will want to or have the capacity to live abroad for several months at a time. So I would like to spread awareness that there is also plenty of work to be done here; you don’t always have to go far away to look for it.
I recently did an interview for the Association of American Medical Colleges (AAMC) because 2015 was actually the first time that all of the positions for OBGYN residency programs were filled in the U.S. I think it’s really encouraging that more people here are taking an interest in women’s health issues. The world needs more providers dedicated to these issues.
Register below for Rachel’s discussion on some of the challenges that keep women in developing countries from getting the medical care they urgently need.
October 21, 2015 – 7:00pm – 8:30pm – Annapolis, Maryland
Check out MSF’s event listing to see when a local MSF field worker will be speaking near you!
#tomorrowneedsher #womenshealth #maternalhealth #OBGYN #sierraleone #southsudan
Because Tomorrow Needs Her focuses on some of the impediments to women’s health, exposing injustices that disproportionately affect women and girls around the world.
In her talk, Dr. Seay will share her experiences in the field with MSF and discuss some of the challenges that women and girls face in trying to access the medical care that they need.
Where have your missions with MSF been and what has been your role in each?
My first mission with MSF was in Fall 2013. The project was in Bo, southeastern Sierra Leone, in a freestanding MSF maternal and pediatric hospital. I was there for about three months working on emergency obstetrics and maternal and child health with two other OBGYNs.
My next project, in South Sudan, was structured a bit differently. There, MSF runs the pediatric and maternity department within a larger government-run Ministry of Health hospital. At this project there is normally one OBGYN at a time who works with an ex-pat midwife, who is supervising and training a larger team of local midwives. My primary role in this project was to work with the midwives and to treat the patients who had complicated obstetrical or surgical cases.
You were recently honored as a 2015 Fellow in the History of American Obstetrics and Gynecology with the American Congress of OBGYN (ACOG). What has been the primary focus in your research to decrease maternal mortality?
Aside from my work with MSF, I’m very actively involved in global health and global health education. I’m on the faculty of Johns Hopkins University where I help with both the OBGYN resident and medical student electives and global health interest groups.
One of my particular areas of interest, both clinically and academically, revolves around the education, prevention and treatment of postpartum hemorrhage. My fellowship research project with ACOG is focusing on the history of the management of post-partum hemorrhage in the United States from approximately 1900-1940. I’m looking at the application of techniques and maneuvers that were used at that time and that might still be applicable in developing and low-resource settings.
In your work on the ground and in your research, what do you see as some of the biggest barriers facing women in terms of accessing medical care?
The issue of women accessing medical care in many MSF-based settings is a complicated and multi-factorial problem. While there are certainly problems in terms of just logistical access, including quality of roads, availability of transportation, and distance from home to a primary or tertiary center, there are also the issues of access related to the prioritization – or lack of prioritization – of women’s health care issues by governments, health administrations, and even health care workers.
Take for example, the issue of how ministries of health prioritize the importance of contraception and prenatal care and how this affects access to those services for women. Meanwhile, I think an additional barrier has to do with the availability of specialized care providers. There is a lack of medical education for general providers with some OBGYN experience and for those with specialty training in OBGYN and maternal health-related issues.
When have you seen these issues of access for women and girls arise in your missions with MSF?
It happens all the time, but there is one story that sticks out in my mind. While in Bo, we had two young girls, both 17, who started off on really parallel courses that ended dramatically differently. Both girls were pregnant with their first babies and had been laboring at home for several days with obstructed labor. Eventually, they each made their way out of the bush to a primary clinic where they were transferred to our facility. By the time one of the girls had arrived, her baby had died, while the baby of the other was still alive. Both girls delivered by C-section and ended up having really bad pelvic and abdominal infections. After about six to eight weeks in the hospital with us, the mother whose baby died ended up dying as well. The mother whose baby survived recovered and ended up doing well and being discharged.
The complications and suffering of both of these girls were happening at the same time – they even shared the same room! To me, this story paints such a stark picture of two different outcomes from a problem that is completely preventable. Both of these girls exemplify the incredible complication and suffering that can come from a lack of access to timely and appropriate medical care. We just don’t see this in developed countries because we have access to quality, timely care.
We also saw a lot of patients who developed obstetric fistulas after suffering from obstructed labor. While our project wasn’t specifically treating those with obstetric fistulas, we would often identify them and refer them to another NGO that was working in the area. Like many complications that I saw result in morbidity and mortality, obstetric fistula is an entirely preventable problem.
As mentioned, often times these issues aren’t as recognized in developed nations because the issue of access doesn’t exist to the same degree as it does in some other settings. What would you hope that people who come to your talk take away from it?
Partly just an expanded awareness of how fortunate we are to have access to medical care, contraception and preventative health care. I would like for the project to encourage people to take responsibility for their own preventative health care and encourage their families, friends and community to be involved as well. Prevention is always better than treatment.
I believe that the improvement of the global maternal health situation is truly an inter-disciplinary effort. And that’s why I’m not only doing talks at medical schools and schools for public health, but also at general universities, not specific to medical audiences.
I think it’s important to raise awareness that there is a need for a lot of different support and skill sets, whether it’s medical or engineering or education. There are many roles and skills needed to improve access to health-related services. I hope these talks will help illuminate these issues, update people about what is being done, and motivate people to get involved – whatever their skill
And I think that traveling abroad is not for everyone, and not everyone who attends these talks will want to or have the capacity to live abroad for several months at a time. So I would like to spread awareness that there is also plenty of work to be done here; you don’t always have to go far away to look for it.
I recently did an interview for the Association of American Medical Colleges (AAMC) because 2015 was actually the first time that all of the positions for OBGYN residency programs were filled in the U.S. I think it’s really encouraging that more people here are taking an interest in women’s health issues. The world needs more providers dedicated to these issues.
Register below for Rachel’s discussion on some of the challenges that keep women in developing countries from getting the medical care they urgently need.
October 21, 2015 – 7:00pm – 8:30pm – Annapolis, Maryland
Check out MSF’s event listing to see when a local MSF field worker will be speaking near you!
#tomorrowneedsher #womenshealth #maternalhealth #OBGYN #sierraleone #southsudan
Because Tomorrow Needs Her focuses on some of the impediments to women’s health, exposing injustices that disproportionately affect women and girls around the world.