



Sexual Violence:
A Long-Term Commitment
Women and Girls, Casualties of War
By Ann Van Haver, Midwife
Beatrice* was one of the roughly 100,000 people who flocked to Mpoko camp in January 2014. Mpoko was the largest of several displacement camps scattered around Bangui, the capital of Central African Republic (CAR). Like many, Beatrice was trying to escape the violence of an ongoing civil war and find shelter for herself and her children.
She had a few items she’d brought with her from her home but little to eat. When she ran out of food, or the children’s clothes got too dirty or torn, Beatrice would have to return home to fetch some essentials. In this lawless context, where armed men were everywhere, that meant taking a huge risk.
“I went back to my house to collect clothes for my children,” she later told me. “I was inside, looking for the things I wanted to pack when I heard a knock on the door. I didn’t dare to open it, and before I could hide, five armed men in military uniform entered the house. They asked where my husband was. I told them he was not there. They pointed guns at me and forced me to lie down. One after the other passed over [raped] me, while two others were pushing me down. Another one told me he would kill me if I shouted for help. After they had finished, they left the house. I felt very tired and lay down to sleep. After a few hours I came back to the camp.”

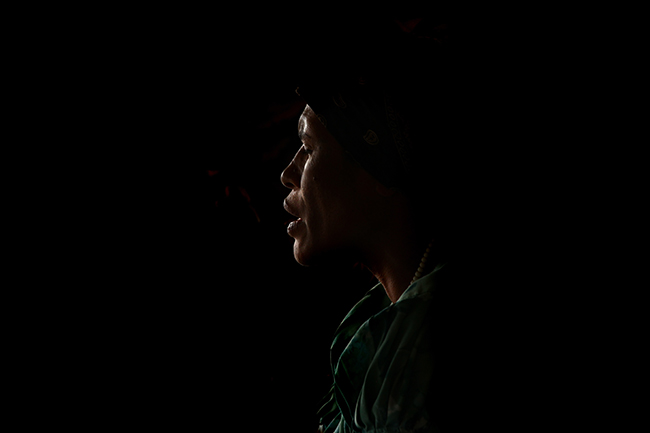
A young woman who was abducted and raped receives care from an MSF midwife and nurse while her mother watches at the MSF hospital in Mpoko camp, Bagui, Central AFrican Republic. Photo by Aurelie Baumel/MSF
For several days, Beatrice had been too ashamed and too frightened to tell anyone what had happened. Then she heard from “the people with the megaphones”—MSF’s health promotion teams at Mpoko—that victims of sexual violence could come to the MSF hospital at the edge of the camp for treatment. That’s where I met her.
Beatrice was not alone in her suffering. During my five-week assignment in CAR, I listened to 31 women describe being sexually assaulted and raped. This was not my first time hearing such accounts, but these women’s stories shocked me. I recount them here because they are both hard to believe and distressingly familiar, because they must be heard and the acts condemned, and because it’s important that people realize that the provision of medical care for victims of sexual violence, while crucial, is only the beginning of what they need.
MSF treated more than 11,000 victims of sexual violence in 34 countries in 2013.
About 95 percent of our patients are women and girls;
five percent are men and boys.
It is MSF’s policy for all projects to offer medical care to victims of sexual violence (Women, men, and children all suffer from these attacks, but the vast majority of victims are women and girls. For the purposes of this book, we will be speaking mainly about them). In CAR, we were in a conflict zone, in a makeshift camp for internally displaced people. As in most conflict settings, our focus was on lifesaving activities, but within three weeks of building a hospital from wood, plastic sheeting and tents, we started a sexual violence program.
I hired and trained a midwife dedicated to treating sexual violence victims, and I recruited three other midwives whom we would supervise. The psychologist at the project hired and trained two female social workers to work in teams with the midwives and to spread the word about our services throughout the camp.
Health care providers can do a lot for patients who have been through sexual violence, although it often seems inadequate for someone who has undergone such trauma. We can treat injuries, prevent or treat infections, manage unwanted pregnancy, offer psychological support, and provide medical certificates.
Stigma and shame, along with fear of repercussions, keep many victims of sexual violence from seeking treatment, however. The path to care must be discreet. At Mpoko, our health promoters distributed small pieces of paper with a referral code to potential patients, who’d then bring it to a female health promoter stationed at the hospital gate. The promoter would escort the patient to the far corner of the hospital, where we had set up a tent that served as the sexual violence treatment area. (We later moved it to an even more isolated area with a fence around it.)
Women who have suffered sexual violence will often come to a medical facility hoping to receive drugs that will let them sleep or alleviate recurrent headaches, body pain, and anxiety. But painkillers or sleeping pills alone won’t help them. A counsellor, a midwife or a nurse will describe how the shock of the violence can cause these symptoms, and how psychosocial counselling can be of service.

A 48-year-old woman who was raped by armed men receives treatment at MSF’s hospital in Mpoko camp. Photo by Aurelie Baumel/MSF
The concept of counselling is often new to the people MSF treats. It is therefore extremely important to create an atmosphere in which a patient feels free to talk, to cry, or to be silent. We work to build that space by first explaining that everything that is said will remain confidential, that we will not tell her story to anyone else, and that we will not judge her. We state as fact that what she endured was not her fault and that we know that she didn’t want this to happen.
Beatrice arrived on the first day we began offering sexual violence treatment in Mpoko. When she was brought in, we asked what had happened so that we could understand the chronology of events and give her proper counselling and treatment. Many victims are not able to tell us everything at first, and we do not pressure them. It can take great effort and courage to revisit these episodes. It can be helpful, but it can also bring back the trauma of the experience. For that reason we ask them to recount their story only once.
For a sexual violence victim to undress
and be prodded by a stranger can be extremely painful and even re-traumatizing.
We therefore we seek approval and involvement at every step of the process.
Before I began the medical exam, I explained what I was going to do. I asked her permission before each time I touched her. For a sexual violence victim to undress and be prodded by a stranger can be extremely painful and even re-traumatizing. We therefore seek approval and involvement at every step of the process. This protocol applies to children as well. If a child victim does not want to be touched, the exam should never be forced.
We gave Beatrice vaccines for hepatitis B and tetanus and antibiotics to prevent sexually transmitted infections. She was still within the five-day window to receive the morning-after pill to protect her from pregnancy, but too late for HIV prophylaxis, which must be given within 72 hours. If a patient has indeed contracted HIV, MSF can offer HIV counselling and testing and connect the patient with HIV services.
“We were hiding in our house when the soldiers came to our area,” Deborah told us. “The neighbors yelled ‘RUN!’ but we were too late. Four heavily armed men were already at our doorstep. My husband hid under the bed, but I didn’t have a place to hide. The men asked where my husband was. I told them he was not at home. The leader decided to rape me. One man forced me down with a knife on my throat. When the other man was on top of me and inside me, he looked aside and saw my husband under the bed. He shot him while he was still on top of me and then continued with me. The other man raped me after him, then they left me unconscious in the house.”

A young woman who was abducted and repeatedly raped is vaccinated at MSF’s hospital in Mpoko camp. Photo by Aurelie Baumel/MSF
Deborah was calm when she came in. She seemed resigned, but the impact of the assault was already apparent. She was having difficulty sleeping and was wrestling with a deep sense of shame. She did not give more details of her story. We asked her, as we ask all sexual violence patients, to return for follow-up sessions so we could continue our work together.
Another woman, Sylvia, who was 24, came in just hours after being attacked. She struggled to find words at first but eventually told us what had happened. She had been selling fruit to earn money. “The man told me I had to come to the [international forces] military camp by 6 p.m., to pick up the money for my fruit,” Sylvia said. “At 6 p.m. it is dark and there are a lot of bandits around the base. The area around there is empty, with bushes. Three men jumped out of the bushes. They took me far away and forced me to have sex with them. They put it in my mouth, in my behind and in my vagina. I fainted. They left me by the side of the road, naked. Two kind people helped me to find my way to the IDP camp. My mother washed me.”
We did not press her for more details, and we gave her the full medical package. We also installed a bed in our sexual violence tent, gave her food, and let her sleep for several hours. When she woke up, we again explained her treatment and her follow up appointments. A psychosocial counsellor walked her back to where her mother was.
In the days that followed, we watched Sylvia closely. She met with our counsellors twice a week. Within a week she was able to function, to talk, even to smile now and then. But she was having flashbacks, sleeping poorly, and was afraid to walk in the street.
Women in areas of conflict,
where there is often a complete breakdown of order,
are particularly vulnerable to sexual violence.
Women in areas of conflict, where there is often a complete breakdown of order, are particularly vulnerable to sexual violence. The threats can come from anywhere: government security forces, rebel groups, militias, and criminal elements that operate with impunity.
If that isn’t enough, rape is often used systematically as a tactic of war, to devastate individuals and communities. During the 1994 Rwandan genocide, between 100,000 and 250,000 women were raped in three-months.i During the Bosnian War, thousands of women were held in “rape camps” and brutalized repeatedly.ii In eastern Democratic Republic of Congo (DRC), where fighting has plagued the country for more than 15 years, around 1,100 rapes are reported every month, with an average of 36 women and girls being raped daily. These are just the reported figures; the real numbers are assumed to be much higher.iii In MSF facilities alone, teams have provided medical care to more than 54,000 victims of sexual violence in eastern DRC over the last decade.

A nurse draws blood from a victim of sexual violence. Her blood will be tested for HIV. Photo by Aurelie Baumel/MSF
Women and girls are vulnerable to rape in other contexts, too—and often similarly hesitant to seek assistance. In Morocco in 2010, MSF teams found that large numbers of female migrants and asylum-seekers from other parts of Africa who were trying to reach Europe needed treatment for sexual violence but were afraid to seek help. MSF and other civil society organizations lobbied the government to improve care for migrants. They also pressed European Union countries to address the effects of increasingly restrictive policies on migrants. In 2011, Morocco passed a law affirming that health care was a fundamental human right for everyone, including migrants.
As a medical organization, MSF’s priority is delivering the targeted medical and mental health care that sexual violence victims need. In certain situations, though, we go beyond that, advocating for changes in policies and procedures that can help facilitate care for those who need it. Morocco was one example. Guatemala is another. In Guatemala City, where violent criminal gangs all too frequently prey on women and girls, many survivors neither report rape nor seek treatment. Those who do may face threats and intimidation.
Claudia’s Mother: “Claudia had told me before that some boys were bothering her and that she was afraid. She went to work one afternoon and then at 6 p.m. I received a phone call. They told me they had my daughter and that they were going to give her back to me some other day, that they were going to have fun with her.
[Several hours later] a neighbor called me and told me that she saw Claudia walking towards the house. She said Claudia was barefoot, her hair was a mess, she looked as if she were drugged. It was very difficult for us to go through those distressing moments, but thank God they gave her back to us alive.
We think this is somebody we know. We made a statement at the police station. Then we dropped the charges for the same reason, because we thought it was someone we know and he might learn about the statement and perhaps do more harm later on.
Nobody informed us about taking her to a doctor. A friend took us to find a hospital but the hospital was no longer where it used to be. We had no idea of what else to do. It never crossed my mind about her having a venereal disease or anything. I was so devastated that I couldn’t think of anything else. We did get her to a hospital, but it was much later.”
Claudia: “A friend of my mom’s recommended the MSF clinic and said we could talk to a woman there. I got all the vaccines against infection and I was screened for HIV. I began with my therapy. It was a very long process. I think the hardest thing at the time was finding out I was pregnant.
We attended therapy every eight days, then we started to have appointments every 15 days. It helped a lot. With such a problem, you can’t do it alone. You need to feel others’ support. Because you really feel very lonely, very abandoned and often very despised because of what you’ve been through. And you feel that it only happened to you.
It was very hard and sometimes very bitter. But I have overcome a lot.
I think the government is not paying enough attention to sexual abuse because they’re more focused on [deadly] violence. They should consider how to help people who’ve gone through this. It’s often not reported and it’s not fully understood. You don’t hear much about it because people don’t talk about it when in fact it’s something that happens every day.”v
As in Morocco, MSF has advocated on behalf of victims, working to make it clear to the authorities, the medical community, and the public in general that sexual violence is a medical emergency and that women who’ve been sexually assaulted must have access to treatment. Teams have also worked with the government and the country’s medical system to improve data collection and case recording.
In cases of sexual violence, MSF offers patients medical certificates. The documents confirm that the patient came to MSF health services and recount the patient’s story and what the staff’s findings were upon medical examination. They do not attempt to confirm or deny rape, but state the patient’s account and conclude whether, upon medical examination, the wounds and the results of the physical examination are consistent with the assault as described by the victim.
Only ten of the 31 women we treated while I was in Mpoko wanted a medical certificate. In conflict areas like CAR, there is simply nothing in place to support victims of sexual violence who want to seek justice. We offer them the certificates anyway in case they decide they want to press charges and there is the opportunity to do so in the future.
Sexual violence spreads unchecked in situations like this,
where the vulnerable can find little protection,
where women and children are assaulted with impunity,
and where the care that they need is too often beyond their reach.
Medical confidentiality, including the safeguarding of medical files and certificates, is critical in treating sexual violence patients. Confidentiality could be compromised at many different points in the recording and storing of information. To prevent this, medical staff need to be trained on how patients should be identified and how much information about them is needed and recorded.
Beatrice was one of the few women I saw who wanted a medical certificate, but her more pressing concern, and that of many other women in Bangui, was how she would feed her family. Most of the women and girls had lost a husband or father and were solely responsible for the children in their families. The camp was not consistently providing food, and making sure their children could eat was a much more immediate worry than legal recourse. What further risks would she have to take?
At that time, MSF teams were conducting around 12,000 medical consultations per week and working to provide water and sanitation services in the camps in Bangui. We were often the only organization providing assistance. MSF repeatedly called on the international community to respond. CAR is still struggling with a complete breakdown of order, and as of late 2014, the UN and donor countries had still done little to address the situation.
Sexual violence spreads unchecked in situations like this, where the vulnerable can find little protection, where women and children are assaulted with impunity, and where the care that they need is too often beyond their reach.

fsc14 copy
“In Tari, Papua New Guinea (PNG), family and sexual violence are very common, but women are much more affected,” said Marlieke de Fouw, an MSF doctor.
All photos by Kate Geraghty

msf2 copy
MSF runs the Family Support Center in Tari, which provides medical and emotional support for patients suffering from family and sexual violence.

fv-tapali7 copy
“Counseling is new to people in Tari,” said Leonie, an MSF counselor from PNG.

fv-marylynpeter20 copy
This patient was brutally wounded during a fight with her husband and a new co-wife.

outreach5 copy
“We go to market every Friday to explain what MSF is, what we do, and what services we provide,” said Dr. de Fouw.

fv-josephinepeterson13 copy
“Four days after we were married,” said this patient, “my husband’s co-wife stabbed me.”

fv-josephinepeterson4 copy
“The physical problem we could take care of, but the bigger problem had not been solved,” said Dr. de Fouw. “ We offered counseling to discuss other ways of dealing with her anger.”

dailylife34 copy
“My brothers have [cut] their wives,” a patient said. “ I get scared [of the violence] sometimes and run away and hide.”

dailylife20 copy
“Some are sad and they struggle to survive. But in general Tari women are very strong,” said Leonie, the MSF counselor.

fv-josephinemichael&mother2 copy
This patient has a bush knife injury on her scalp.

dailylife17 copy
“I have a son,” a patient said. “I will talk to my son and tell him not to hit women and not to kill men and not to steal.”
A Scourge in “Stable” Places
By Rebecca M. Singer, RN, ND
It was towards the end of the day at our clinic in Lae, the second-largest city in Papua New Guinea (PNG), when Jennifer came in. She had been absolutely brutalized, beaten all over her body and badly wounded. Jennifer told us she had been gang raped at a bus stop in the middle of town. Six men had attacked her on her way home from work. She knew some of them.
We cleaned her wounds, gave her prophylaxis against pregnancy and HIV, and told her she needed to come back to continue the HIV medication. “I can’t,” she said, “I just can’t.” She was ashamed that such a thing had happened to her, and she was afraid. She didn’t want any more trouble. She wanted to put the whole thing behind her.
We begged her to come back. Finally she gave us her phone number, and we gave her a ride to her destination. We tried to follow up with her, but we never saw her again.
A woman sings Tari, Papua New Guinea (PNG), where MSF opened a health center for sexual and family violence. Photo by Kate Geraghty
Jennifer said she felt alone in her experience. But her injuries, mental trauma, and sense of shame are shared by millions of women and girls who have suffered rape or sexual assault around the world. And not just in war zones. MSF also works in so-called stable settings, places where there is no active conflict but sexual violence is still a constant threat. PNG is one such place. South Africa is another; according to a study released in 2011, in fact, more than one in four men in South Africa said they had committed rape.iv
There is limited information on rates of sexual violence in PNG. Research conducted by Papua New Guinea Medical Research Institute in 1994 is the most commonly cited. Fifty-five percent of the women in the study said they’d been forced into sex against their will, usually by men they knew. Half of the married women surveyed said their husbands used beatings or threats to force them into sex. Sixty percent of men in the study said they’d participated in gang rapes.v But—and here is where the similarity to war zones comes in—women and girls in PNG can only rarely access medical care for their injuries or risk of infection. There is also very little social or psychological support for mental trauma and few legal avenues through which the perpetrators might be brought to justice.
“I live in an outlying neighborhood between two very dangerous districts. [After a girl was raped by intruders in her house] our neighbors got together and made a team to watch the neighborhood. Then two sons of people in the team were killed. So, they decided to stop watching. Then the “mareros” [members of the Mara Salvatrucha gang] took over the neighborhood.
I was walking to work at 5 o’clock in the morning when a white sedan with tinted windows stopped next to me. They rolled down the window and pulled out a gun and told me to get in. I tried to keep walking and the car kept moving backwards. They said, ‘get in or we shoot you.’ A man got out and put me in the car. They put tape on my hands and mouth and told me if I screamed they’d kill me.
They took me to a hotel. They were getting high and then they undressed me, started stroking me, kissing me. I asked them not to hurt me. They put me on the bed and began to have sex with me. After one got up, I tried to get up, and they pushed me back on the bed. Then it was the turn of the other one.
Afterwards I saw him going to the table where the gun was. I begged them, ‘I have children, please don’t kill me.’ He said, ‘I’m not asking you. Shut up.’ He put the gun on my forehead. I felt like dying. I just closed my eyes and he said, ‘If you speak, I’ll find you anywhere and I’ll kill you.’ I stayed there I don’t know for how long. One of the hotel maids came in, then another girl came in and they helped me get dressed. They talked to me but I couldn’t say anything. I began to cry, calling for my family.
When I got home I was so angry and I didn’t want to leave the house. I didn’t receive any medical care at first. Later, when my family took me to go look at photographs to try to identify the men, someone told my mother about MSF.
We went to MSF and they gave me medication and tended to me and I started receiving counseling there. At first, I couldn’t speak. I couldn’t tell what had happened because I was terrified. There was a time when I thought of ceasing to exist. Thanks to the therapy, I have gotten better. I will continue with it until I really know I’m fine. I have to heal that memory so that it no longer mortifies me.
I stayed alive because there are other people who are killed. There are women who are raped and remain silent and don’t seek help out of fear or shame. But we all know that [rape] is not something that we seek, but something they force us to do against our will.”
In 2010 and 2011, I spent five months working in Lae as the project coordinator of MSF’s program for victims of sexual and family violence. It was a unique program for MSF, one of the very few projects that specifically reaches out to victims of family violence, along with victims of sexual assaults. People wounded in family violence constituted most of the cases we saw, though we also treated many women and children for sexual violence—2,894 in all, between 2007 and 2013.
During my assignment in Lae, I came to realize that managing the medical care for victims of rape is the easy part. It’s everything that comes before and after that is so complicated. As Jennifer’s story illustrates, follow-up is a constant problem that can have severe consequences if it does not happen. Post-exposure prophylaxis for HIV is a 28-day course of treatment, for instance. MSF has seen that if patients are given the entire course of drugs at once, only half of them will complete it, so we try to get victims to come in again. The patient also needs to come more than once for effective tetanus protection; patients with hepatitis B must come back for a second and third shot.
Most patients never return at all, though, and thus never finish their treatment. When possible, MSF uses community health workers to find patients who miss follow-up appointments and try to persuade them to come back. This works with some, but not all.
There are many reasons why women may not return for follow-up. In places such as DRC, travelling means risking getting robbed or even raped again. Women in rural areas, far from the nearest treatment facility, may have no access to transportation. Another reason stems from a lack of understanding about the importance of the care. The value of a woman’s or girl’s health and well-being are not seen as high enough to offset the cost of receiving this care—whatever that cost may be.

A woman recovers at the Family Support Center in Tari, PNG. Photo by Kate Geraghty
In any context, a rape victim faces the risk of being identified. A woman who is not pregnant and is making many trips to the hospital could be talked about, and the fear of stigma and its social repercussions could be a price she does not want to pay. It’s hard enough convincing women to come in for treatment the first time. Asking for a second or third visit only compounds the difficulty, no matter how necessary we tell them it is.
Perhaps the strongest barrier to victims receiving care is the shame that is so closely linked to rape. This is something I see in the U.S. and in the field alike. It’s global, this immobilizing feeling that somehow the victim caused the rape to happen and must bear the consequences. When I worked with MSF in Liberia, a patient told me, “If you’ve already had sex and consented once, there is no such thing as rape after that.” I also heard, “Well, I’ve been raped before, so…” It was as if it happened once, the next time it wouldn’t matter.
“My attacker was my own husband. I was working the night shift. I had been trying to stay away from him and he started chasing and following me.
One day in November my children asked me for permission to go to their aunt’s place for the weekend and when they went, they left the door open. That is how he came in. When I arrived home, he was already there and I didn’t realize it. I went to bed and that is when he attacked me. He waited until I fell asleep.
Afterwards I didn’t do anything. Mostly out of fear or shame. What I did was lock myself in my house. I didn’t look for any kind of help from anybody. I stood right there, stuck. It was three or four months before I went to the health center.
I didn’t know about the need to go to a doctor within 72 hours. If I’d known, I would have gone. I didn’t go until I couldn’t bear my own burden or my own guilt anymore. I felt guilty, mainly because I thought, ‘if maybe I had noticed [that he was in the house], it wouldn’t had happened.’ The day I came to the health center was a horrible day. I felt bad, I just cried. I felt worthless, like nobody. I was nothing.
Before, I didn’t leave my house. I didn’t take my children to school. I didn’t check on how they were doing. I was fired from the place where I worked because I lost control in such a way that I couldn’t work anymore. Before this happened, I used to interact with everybody. Now I’m like this. I stand aside. I used to have friends, but it’s not like that anymore.
At the beginning, I had to come here on foot and that was very difficult, but I wanted to move forward. I wanted to get better, to overcome what had happened to me. I have moved forward thanks to the support of the doctors who treated me during those difficult times.
At first, I couldn’t accept what I was bearing in my womb. I didn’t want him. Nine months passed and I couldn’t accept that I was bearing a child. I was scared. I was afraid of looking at him after he was born. But thanks to the help I received, I could overcome it. When I saw him, I felt love for the child.
I feel I just need to do my part and here I am, working hard on that. Because that’s my best wish, having a job to support my children. They depend only on me. They get no other help.
The truth of the matter is that we can’t live like that. It is painful. It’s something that affects you psychologically, and it not only affects the person but the whole family. I feel it affected my children. Even though they don’t know anything, it did affect them as well.”
When I worked in Liberia, there was a night when a woman named Marie was brought to our clinic in very bad shape. She had been gang raped after she went out dancing with her friends. She told me her story: she worked as a prostitute but that particular night she was just out to have a nice time. Now she didn’t want anyone to know what happened, she said, because in her neighborhood, prostitution was accepted but rape was shameful. What’s more, like many survivors of sexual violence in Liberia, Marie did not want to go to the police, either. This was a common sentiment; I heard many Liberian women say that they feared retribution should their attackers learn that their victims reported the crime, and that they feared the police themselves, too. In Liberia (and in PNG, and other countries), women all too often were raped again by the very policemen to whom they reported the initial crime!
Sex crimes against children also go unreported. Children make up roughly half of the victims of sexual violence that MSF sees. In Lae, half the rape survivors we saw were children; among girls the median age was 13. In Liberia the figure was around 80 percent with a median age of 13 for girls and 10 for boys.

A newspaper clipping is taped to the wall of the center while a woman waits to have her wound dressings changed. Photo by Kate Geraghty
Children often don’t tell anyone about the crime because they are afraid of what might happen to the perpetrator, who may be a parent or neighbor. They may also be intimidated into keeping quiet. Family members may not want to confront each other even when they know what has happened, or they don’t want to endure the stigma or the prospect of inviting retribution against the attacker, who might be the husband, brother or uncle, and also perhaps the breadwinner for the family. We saw many families in Liberia and PNG who brought their children in for medical care but would not report the rape to authorities.
It can be very difficult to help remove a victim of sexual violence from danger at home. In both Lae and Monrovia, there are few if any safe houses, and neither city had well established child protective services. This meant that people usually had no choice but to return to where they were abused.
Sexual violence must be acknowledged in a community
for things to start to change.
The establishment of access to safe termination of pregnancy is another challenge. Women and girls who are raped and become pregnant are twice as likely to have an abortion,vi and in places where abortion is legally restricted this can be extremely dangerous. In Liberia, we saw many pregnant teenage girls who said their pregnancies were the only reason they told anyone that they had been raped. In hopes of terminating the pregnancy, many had done terrible things to themselves—inserted sticks or lye into their vaginas, for example—or had paid someone else to do it for them. There was something in Liberia called an “RPG,” as in rocket-propelled grenade: a combination of herbs and lye and chemicals that they would insert into themselves. Frequently these attempts would go horribly wrong, and the girls and women would come to us badly wounded or very ill, some with life-threatening injuries.
Incidents like these, which occur in numerous countries around the world, show how important it is that safe abortion services are made available. As we saw repeatedly, the alternatives can be fatal.
As difficult as it can be to persuade victims of sexual violence to come for medical services, we know community outreach can work. After we let people know where to come for care in Lae, patients started arriving. We had billboards in town, we did radio shows, and made weekly visits to community markets and churches to spread the word that victims of sexual violence should come get treatment within 72 hours of the attack.
The more outreach we did, the more women and girls came in within those crucial 72 hours. We knew this wasn’t everyone, but it was a good start. Sexual violence must be acknowledged in a community for things to start to change. In 2012, the third year of MSF’s program in Lae, after we’d conducted outreach and advocacy, we noticed an enormous change in how society talked about violence, including rape. More people in the community, in parliament, and the Ministry of Health acknowledged the problem and called for action.
However, a major barrier to expanding community engagement is the lack of existing data—numbers that can reinforce the demands for change. MSF can point to the numbers of patients treated at its projects in PNG, but there are no recent official numbers on the prevalence of sexual violence nationwide. Reporting methods in the country must change for the government to get a clear picture of the extent of sexual violence.
The issue extends beyond PNG: currently there is no reliable way to know how many women, men and children have suffered sexual violence around the world. The closest study we have is one published by the WHO in 2013 that looks at violence in general. It found that around 35 percent of all women “will experience either intimate partner or non-partner violence,” which includes but is not limited to sexual violence.vii We lack a study that shows the scope of the problem of sexual violence, which makes it more difficult to press the international community, governments and communities to take action.
Changing systems and policies and reducing the stigma carried by victims of sexual violence requires time, resources, and political will. To start the process, treatment and support must be made available to anyone who needs it. And when care is available, people must know how to gain access to it. In Liberia, for instance, MSF’s small, three-person medical and mental health team saw 150 victims of sexual violence per month due to our outreach activities. But we know that was just the tip of the iceberg.

An MSF outreach team heads to the market in Tari to tell the community that there is treatment available for sexual violence. Photo by Kate Geraghty
You Are Not Alone
By Aerlyn Pfeil, Midwife, CPM, BSM
In 2013, I was working in Wardher, a town in Ethiopia’s Somali region. One night, I woke up to hear a woman screaming, clearly in distress. Then I heard other voices, another woman yelling. I remember thinking it sounded like a woman was being raped and murdered. It was horrible.
There are many different armed factions fighting in this volatile, perpetually neglected region of the country. It’s a place where women and girls are extremely vulnerable to rape and assault.
The sounds were coming from directly behind the walled MSF compound in the village. The MSF guard came to ask me if he could go see what was going on; by then, we had also heard gunfire. I was too worried that something would happen to him if he went, so I told him not to. Unless someone came to us to get help, we’d have to wait and see what happened the next day.
In the morning, we found out that a woman I knew, Hannah, had been attacked and that she and her children had been detained. I got permission to bring her some medication and to have a brief private conversation with her. After she was finally released, we talked more. She told me that she wanted me to share her story.
Unmarried women and girls who are raped lose value
as potential wives—they may even be forced to marry the perpetrator.
These social dynamics make it extremely difficult for victims to seek care.
A man who belonged to an armed group and lived not far from her hut had broken in and sexually assaulted her and her daughter. When they could, Hannah and her son fought back, eventually chasing the man out of their house. The man then fired his gun to alert other men from his group to come, but luckily no one did. The police came the following day and took Hannah and her children to jail.
Hannah’s attacker turned up at our emergency room seeking treatment for his head injuries. (I was working in the maternity ward and did not see him; to practice the MSF principle of neutrality in this instance would have been extremely difficult.)
The assault on Hannah and her daughter was among the most disturbing events that occurred during my time working with MSF. With incidents like these, there was nothing I could do except to help the victims as best I could, giving them the best possible care. But this effort comes with huge challenges.

MSF’s health facility in Wardher, in the Somali region of Ethiopia. Photo by Judith Starkulla
MSF supports several departments of the hospital in Wardher, offering antenatal care and maternity services, treatment for severe malnutrition, and pediatric care. It also runs the emergency room and the tuberculosis (TB) ward. The staff sees two to three victims of violence-related trauma every day—mostly people with wounds from gunshots, knives, burnings, or beatings, along with victims of sexual violence, most of whom are girls under the age of 18.
In 2013, the team treated 33 survivors of sexual violence and five others who the team suspected had been raped. The patient numbers alone give the deceptive impression that sexual violence is not a major issue in Wardher. But after conducting interviews with the community that year, the maternity team estimated that less than 10 percent of sexual violence survivors in the area sought care.
In Wardher, rape is defined as forced sex outside of marriage (rape between husband and wife is not acknowledged). Unmarried women and girls who are raped lose value as potential wives—they may even be forced to marry the perpetrator. These social dynamics make it extremely difficult for victims to seek care.
As in Hannah’s case, husbands and fathers often migrate to other parts of Ethiopia or Somalia to find work and women and children are left alone. Children are frequently charged with tending livestock and collecting water by themselves. Many women and teenagers told us that armed men go house to house and ask the children if the father is home. If he is away, they will return to harass and rape the women.
“Our journey is not the journey that others see. When you are alone, when you don’t have anywhere to sleep or you don’t know the country; you are exposed.
In Tamanrasset, they take the women, search them one by one, undress them and rob them, take their mobiles, their money, even their dresses. And if they like you, they have sex with you.
We stayed there, and then they tell you they want to help you, but then when the night comes, then they start the job on your body. They beat you. They do what they want. If you don’t want to, they make you leave and the police come and take you.
I don’t know if it was the second or third rape. I have to tell [my son] the truth. You can’t hide it. It’s a story that I will always tell, even if I go to Europe and one day I get married, I will always tell my story.”
Beauty, 32, left Ivory Coast during the 2011 war there. She says her name was on a list of those supporting the wrong man for president. She witnessed members of her family being killed. Beauty left her child with her father, who was not politically marked, and set off for Europe. In Tamanrasset, Algeria, she said she was raped by two men.
“He covered my mouth with his hand and he raped me. Then the other one came and raped me. They did it again and again, two people taking turns. I was suffocating and lost consciousness. When I woke up I was all wet, they had thrown water on me. I couldn’t speak. They dressed me and took me to the place where they had caught me. They left me there.”
When she was in Maghnia, near the Moroccan border, she was raped again. She was tricked by a seemingly friendly woman who brought her with some friends to a house.
“After getting there, they locked the door, they gave me a blanket, and I thought that maybe they are kind. But that night they started raping me.”
Beauty became infected with HIV and tuberculosis. She received medical and psychological care from MSF in Rabat, Morocco. She hopes she will recover from TB and get healthy again.
“In my country if you have HIV you are isolated, you are marginalized. You have become the black beast. If I was not been killed in my country, or on the way here, and if this disease has not killed me, it is because God has something in store for me and wants me alive.”
Aimee was raped by armed men during the 2011 war in Ivory Coast. She left and worked for a year at a restaurant in Mali, which was also threatened by war. She decided to join a group of people heading for Europe. During the journey, the man who had organized it took her as his “wife.” When they arrived in Algeria, she was sold to the man’s friends.
“He said, ‘She is my companion, I have bought her. You can do with her whatever you want.’”
Aimee was then forced into a human smuggling network. She was sexually exploited and forced to work as a slave.
“I was there six months. The work we were forced to do was very hard. We had to fill sacks with sand and carry them, take very big stones and drag them. It was very difficult, but if you failed to do it, you weren’t given food. And if you refused, they raped you again.”
Aimee made it out and went to Rabat, Morocco. Many African women are forced into prostitution in Rabat, but she is not going to be one, she says. Her dream is to get to Europe and start a chain of beauty salons.
One woman we met, Ruth, lived in a tiny hut with five small children whose father had not been around for months. “The men know I have no husband,” she told me during a visit. “They come into my house in the evening and they drink all my water, all my tea, they eat all my food, and they can do whatever they want. I have no power.”
Ruth had not been raped, but she said she would be eventually and she knew she would have no recourse. “What can I do?” she said. “These are the people who supply my water. These are the people who are supposed to protect me.”
In Ethiopia as in numerous countries, it is difficult for women to come into a hospital and say, “I have been raped. Please help.” In Wardher, doing so could be dangerous. Knowing we had to work with these realities, we concluded that the best way to reach women and provide them access to services for sexual violence was to go to them, in their homes and communities.
In 2014, during my second assignment in Wardher, our small sexual violence team initiated a form of private, home-based care for survivors of sexual violence. We went from house to house in town, giving health information talks. While speaking with groups of women, teenagers, men, and community elders about why they should vaccinate their children and why women should come to the hospital when they’re in labor, we also talked about sexual violence. Including the topic in a broader discussion about health made it more acceptable, less intrusive. This gave us more space to talk about the potential medical consequences of rape and the confidential services available at the hospital.

A girl stands among huts set up by displaced people living around Wardher. Photo by Will Robertson/MSF
The talks allowed the team to gather a lot more information. We learned that the perpetrators women were most afraid of were “those with guns.” They could be soldiers, the militia, rebels, or other armed groups; the women were hesitant to make a distinction. But it was clear that women were more comfortable coming to the hospital if they had been raped by a civilian as opposed to an armed man.
In recent years, three Ethiopian staff members in Wardher had travelled to Nairobi to receive MSF’s international training on sexual violence. Those staff and I trained the other midwives and community health workers to identify signs and symptoms of sexual violence, and how to provide basic counselling. The training emphasized how to talk about sexual violence in one’s own community, and we encouraged them to use the appropriate messages. They ended up writing a song in which they described the health consequences of sexual violence. For these Somali women, who don’t speak about such things very often, it was a pretty powerful song.
Once we started to direct attention to the issue, we saw growing interest in it. Each week, we met with local groups, including traditional birth attendants, to get our message out and keep the conversation alive. More talking did not necessarily translate into more care, though. As of mid-2014, the number of victims coming in had not risen much.
I am also a survivor of sexual violence and I didn’t get medical treatment. I didn’t seek legal recourse, and my life wouldn’t have been at risk if I had. This is why I knew that we needed to be patient. I want to see organizations like MSF and national health systems make a difference for these women, but care providers have to commit to the process and understand that it will take a lot of time, training, and sensitivity. Everyone must examine their own discomfort with the subject of rape. The messages will need to be repeated constantly.

Displaced women in Wardher gather together. Photo by Will Robertson/MSF
For an emergency medical organization like MSF, it can be difficult to prioritize a problem as hidden as sexual violence, especially when so many other issues need attention. It is just as easy for governments to overlook sexual violence. But the problem is there.
Another challenge that is not widely understood is the reoccurrence of trauma. Many of the staff who work in these programs have social and economic circumstances similar to our patients. The female staff I worked with in Wardher expressed the same fears of violence. They felt at risk. Victims of sexual violence may heal physically, but the pain will always be with them. If a female health worker is caring for victims of sexual violence, her own experience with sexual violence could surface, and she will need support.
Even staff who have not suffered from violence first-hand face the effects of suffering or trauma. Health care providers can do a better job of helping staff recognize their own sources of anxiety and distress, and then supporting them.
MSF cannot prevent violence.
But our care providers must be creative
to find ways to reach women. We still have a long way to go.
Lately, the situation with armed groups in Wardher has worsened, and the lot of women there has worsened along with it. As in all our programs, MSF cannot prevent violence. But our care providers must be creative to find ways to reach women. We still have a long way to go.
MSF began treating victims of sexual violence 15 years ago when the organization recognized how simple interventions such as prophylaxis for HIV and unwanted pregnancy could keep patients from suffering even more. The obstacles to providing treatment remain enormous. At MSF projects, teams focus on areas where they can make an impact: ensuring confidentiality, encouraging people to come early for treatment, and convincing patients to get follow-up care. MSF also advocates for and at times provides direct assistance to help governments recognize sexual violence as a medical emergency and improve treatment and reporting systems.
But among the most challenging aspects of responding to sexual violence is dealing with stigma and shame. They enable rape because they keep victims silent and afraid. In some cultures, the social rejection that follows rape has the potential to cripple victims for the rest of their lives. It is no wonder sexual violence remains a hidden problem.
As with so many other difficult challenges, governments, health authorities, MSF and other health care providers must commit to working against sexual violence by reaching out to victims in any setting. While MSF projects are likely to see only a fraction of the people who need treatment for sexual violence, we have also seen that in providing the care, and in talking about the issue again and again over time, more women, girls, men and boys will seek the care that they need.
*Patient names have been changed.
iOutreach Programme on the Rwanda Genocide at the United Nations. Background Information on Sexual Violence used as a Tool of War. Accessed December 2014. http://www.un.org/en/preventgenocide/rwanda/about/bgsexualviolence.shtml
iiConflict Profile: Bosnia, Women Under Siege Project. Women’s Media Center. 2012. http://www.womenundersiegeproject.org/conflicts/profile/bosnia
iiiEnding Violence Against Women and Girls,” United Nations’ Resources for Speakers on Global Issues. Accessed December 2014. http://www.un.org/en/globalissues/briefingpapers/endviol/
ivRachel Jewkes et al. “Gender Inequitable Masculinity and Sexual Entitlement in Rape
Perpetration South Africa: Findings of a Cross-Sectional Study.” PLoS ONE. December 28, 2011. http://www.plosone.org/article/info%3Adoi%2F10.1371%2Fjournal.pone.0029590
vAmnesty International. Briefing to the UN Committee on the Elimination of Discrimination Against Women, p. 9. 2009. http://www2.ohchr.org/english/bodies/cedaw/docs/ngos/AI_PapuaNewGuinea46.pdf
viWHO Fact Sheet. Violence Against Women, updated November 2014. http://www.who.int/mediacentre/factsheets/fs239/en/
viiIbid.